Centre for Personalised Medicine Art Competition 2025-26
Earlier this year, the CPM ran an art competition asking UK students in Years 7 to 9 (approx. 11 to 14 years old) to send in art exploring the meaning of ‘personalised medicine’ and showing us what it meant to them. You can watch a video introducing the competition here.
We were thrilled to receive almost 100 entries, which were judged by Dr Rachel Horton (CPM Affiliate Member), Francesca Dakin (CPM Junior Research Fellow), Honor Davies (Oxford University Personalised Medicine Society), Dr Jason Waite (History of Art, St Anne’s College) and Dr Naomi Marshall (Clinical Ethics, Law and Society group, University of Oxford).
This blog showcases the artwork of our outstanding winners and finalists.
Winner: individual category

By Frida, age 14, Fallibroome Academy, Macclesfield
Frida explained that her artwork ‘represents personalised medicine as layers of digital tabs made using plexiglass and a doctor and patient on either side. Each layer representing information that helps the doctor understand the patient as an individual. The stacked tabs show that medical decisions are made using many factors. I used these tabs to show that personalised medicine means building care from many factors. Using this information helps doctors choose safer and more effective treatments to tailor care for each individual patient.’
The judges thought this was a brilliant and imaginative concept: the idea of a doctor having to ‘look through’ layers of information before finally seeing the patient was very compelling. We really enjoyed the use of layered panels, adding a physical depth that cleverly mirrors the concept of layered data. Frida’s entry really stood out for its creativity, originality, and clear communication of a complex idea.
Joint runner-up:

By Nyah, age 12, Channing Senior School, London
Nyah described how her artwork ‘summarises what I know about what personalised medicine is and how it produces a more accurate diagnosis by using your unique genetics, lifestyle, and clinical data to tailor healthcare.’ She wanted her artwork to ‘tell the story/journey of somebody who has decided on having personalised medicine and show what the process can be like. I have depicted a young girl receiving a sample of her medicine. She had to attend multiple appointments and the scientists also had to perform many tests. DNA plays a vital part in how personalised medicine is designed and so I also wanted to spotlight this. I thought about what DNA is made from and what it does for medicine. It is represented in my painting as a staircase with family members watching from it.’
The judges thought this was a beautiful and powerful entry that clearly reflects a great deal of effort and thought. We were really impressed by how the composition cleverly brings multiple elements together, demonstrating impressive artistic skill along with a strong level of research and understanding.
Joint runner-up:
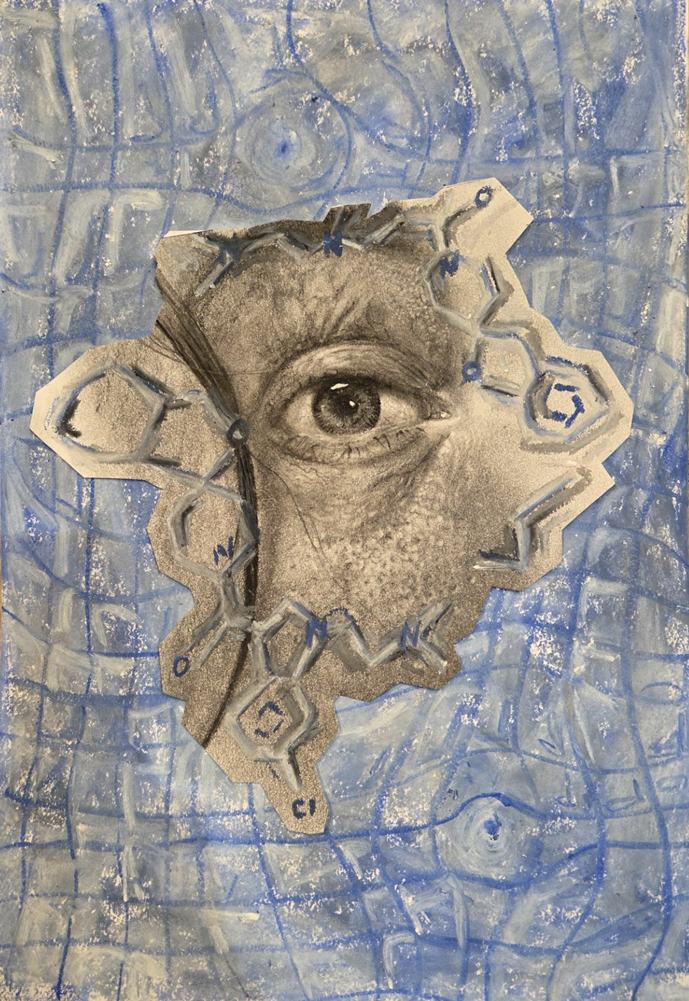
By Millie, age 14, Beckfoot School, Yorkshire
Millie said, ‘my picture is a charcoal drawing of an eye displaying the chemical structure of Faricimab, a medicine used to treat age related macular degeneration. The background shows the type of vision that people with AMD can have, overlaid with an Amsler chart, which people can use at home to see whether their eye disease is deteriorating or staying the same. Faricimab isn’t suitable for everybody, for those who can use it, it’s sight saving and the impact it can have is amazing!’
The judges loved how Millie’s detailed charcoal drawing of the eye draws the viewer in, while the inclusion of a real drug structure and the distorted background clearly communicate how personalised medicine targets specific conditions like vision loss. We thought Millie’s decision to include the Amsler chart and visual distortion was especially effective in helping the viewer understand what patients experience, not just the treatment itself.
Highly commended:

By Gagan, age 13, Sutton Coldfield Grammar School for Girls, West Midlands
Gagan wrote that ‘the hands holding prescription bottles acts as a metaphor for individuality as the labelled medicine highlight how medical treatment is tailored to individual needs rather than a single “perfect” solution. The circular composition symbolises equality and humanity, while the imperfect spacing reflects how people do not fit neatly into scientific categories, and should not be defined by data.’
The judges thought that Gagan’s artwork was beautifully artistic and very thoughtful, conveying how people’s different needs and priorities might influence prescription.
Highly commended:
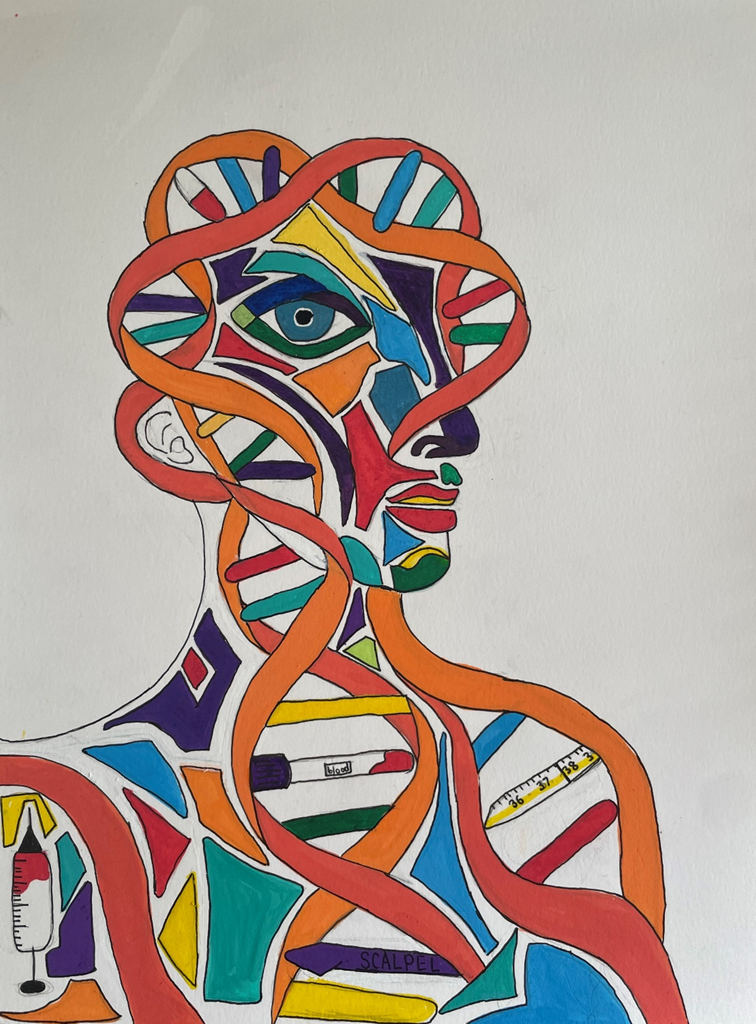
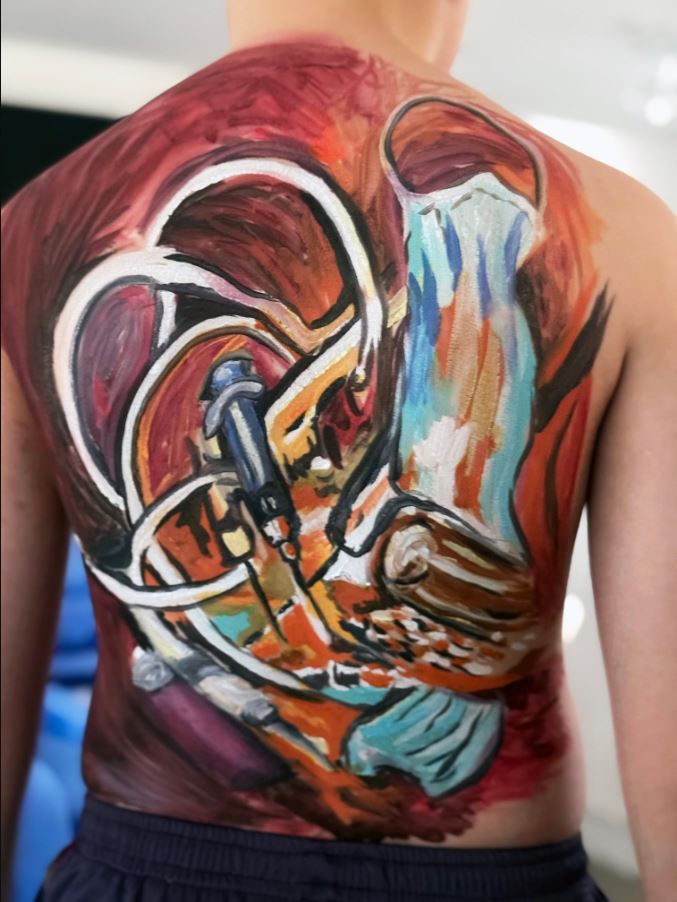
By Ottilie, age 13
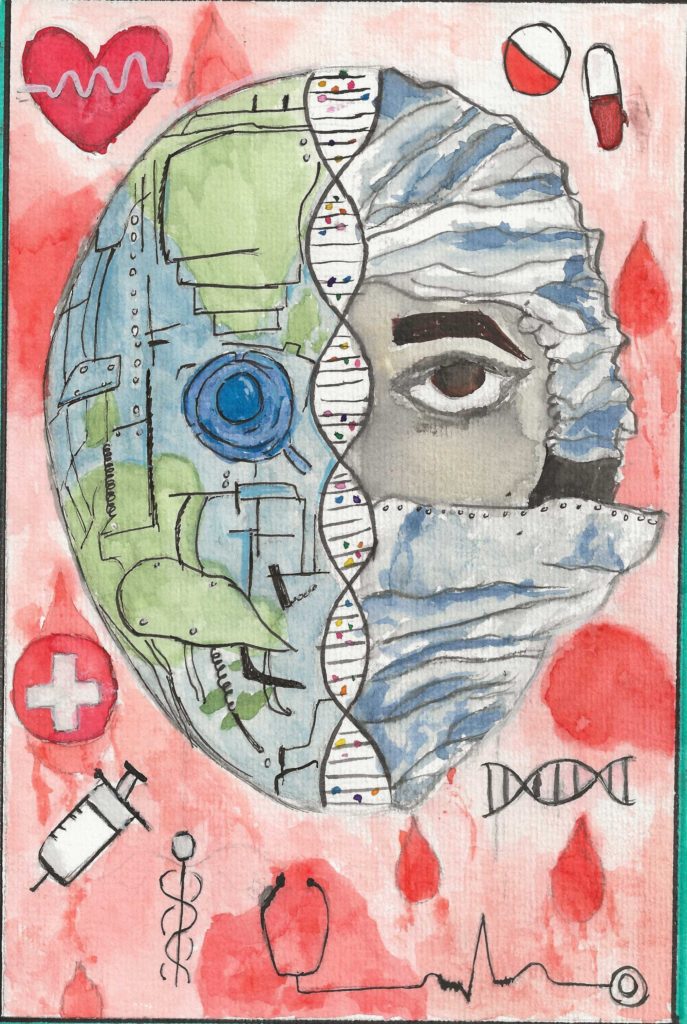
Ottilie’s artwork is titled Tailored Treatments. She wrote ‘I have drawn it in an abstract style as I think this best represents the uniqueness of the individual and how care should be tailored to their needs. The image I created is composed of DNA double helix with medical equipment interspersed in its structure to reflect the increasing ability of personalised medicine to treat people at a genetic level. The lines that form the person are smooth and flowing, emphasising the fact that we are not just DNA but unique individuals that need kindness and care when we are ill. I used bold colours so that every person should be seen and stand out.’
The judges really enjoyed this bold and original artwork, and thought it had a strong artistic identity. The abstract style of this piece was really striking and it was clear that a lot of thought had gone into the details. We thought it showed mature thinking about how art and meaning connect.
Highly commended:
By Darcie, age 13, Didcot Girl’s School, Oxfordshire
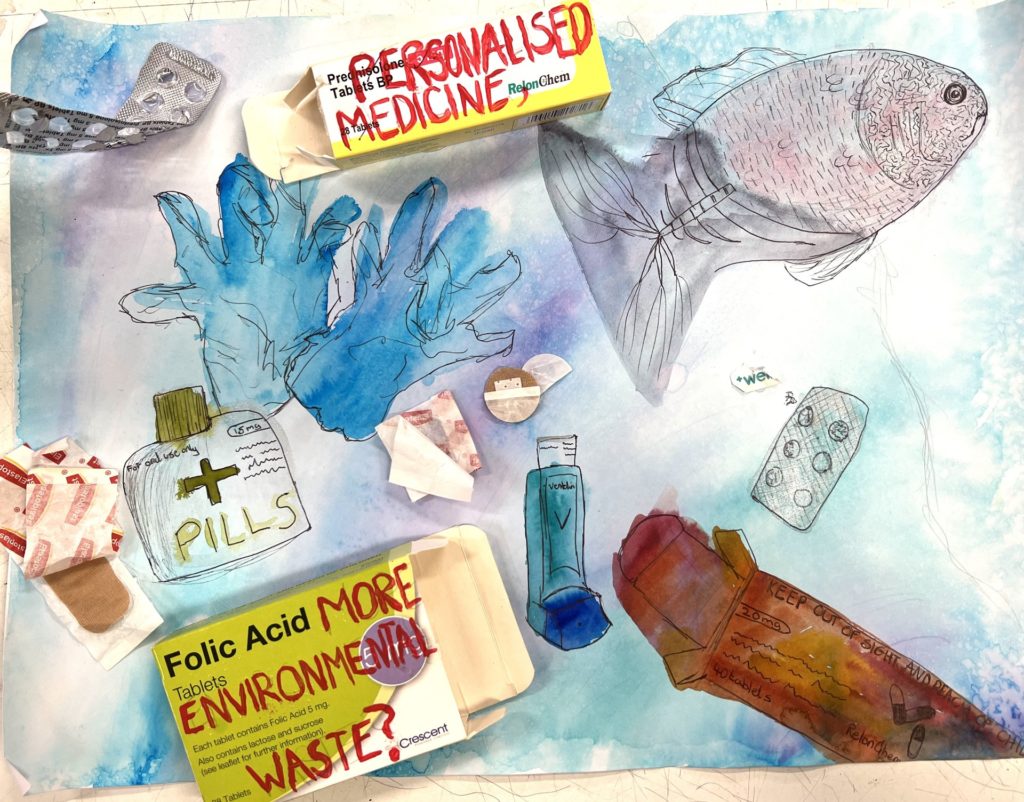
Darcie’s artwork was based on a loved one’s experience within the medical world, and her personalised medicine. She wrote that she ‘wanted this artwork to highlight the struggles she goes through but also what all the doctors do to keep her healthy. Displayed is some of the medication used e.g. the inhaler and montelukast. She has monthly injections to help her with her asthma, hence the needle. The different shades of the lung show how quickly someone’s state can change with asthma, all the things that can cause complications within the lungs.’
The judges loved this very raw and personal account of personalised medicine: we thought it was a strong and thoughtful interpretation that clearly shows how medicine is tailored to one person’s needs. We thought the personal connection made this piece very powerful, bringing empathy and emotion into science.
Highly commended:
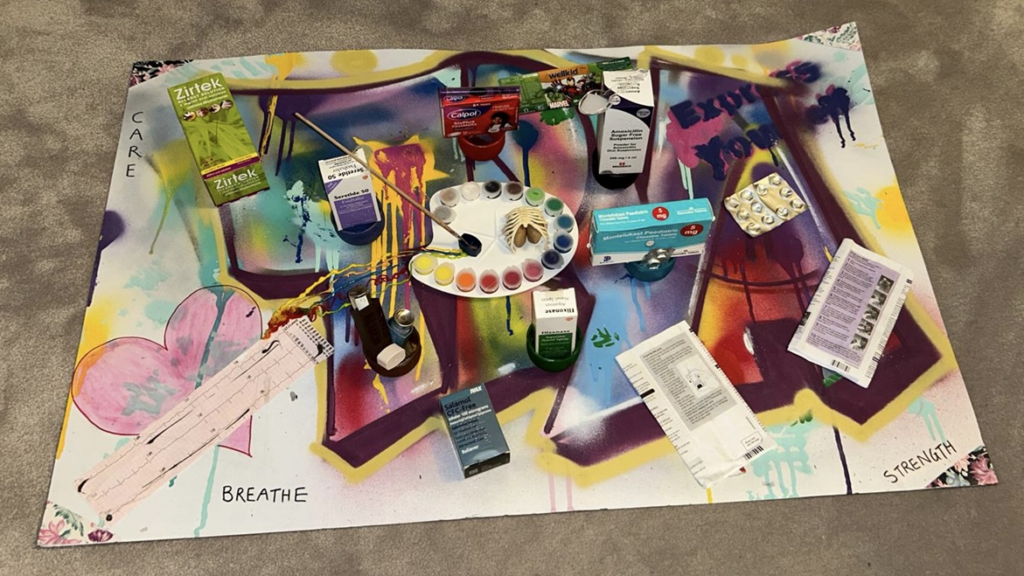
By Tiya, age 13, St Helen’s School, Northwood
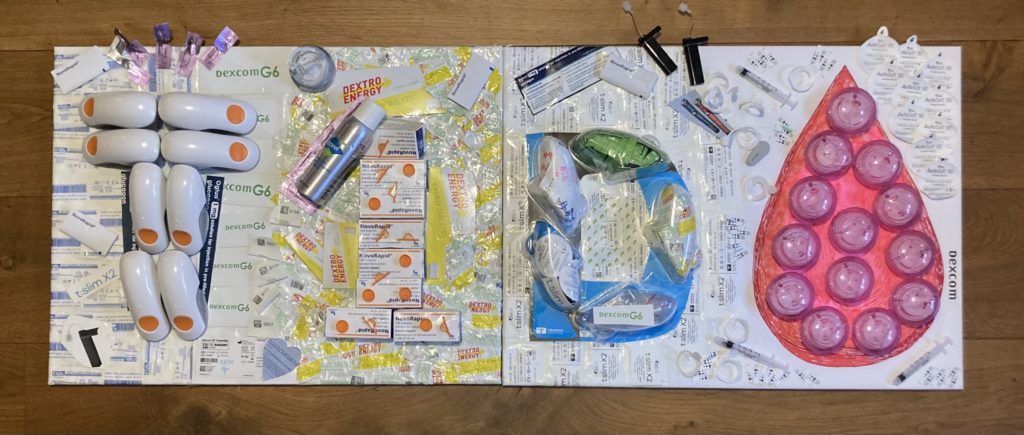
Tiya’s artwork ‘represents personalised medicine as something unique and individual … The doctor’s palette, at the centre, symbolises how doctors “paint” medicine by combining care, treatment, and data, to meet a person’s healthcare needs. Surrounding the palette are pots of paint, containing boxes of medication, along with blister packs, instructions, and wrappers, reflecting the reality of managing health daily. The lungs at the centre represent living with asthma. A paintbrush tipped with an inhaler cap blends a trail of colours towards the heart, showing how treatments work together to support health. The ECG strip and heart represent monitoring and protection, while the words “breathe” and “strength” highlight what personalised care allows. In the background, graffiti formed from my name and the phrase “Express Yourself” shows that identity, creativity and self-expression are essential parts of healthcare.’
The judges loved the individuality of this piece. We really liked the concept of the doctor’s palette: it was such an evocative way of thinking about the delivery of personalised care. We were also impressed with Tiya’s repurposing of waste materials to create this powerful artwork.
Highly commended:
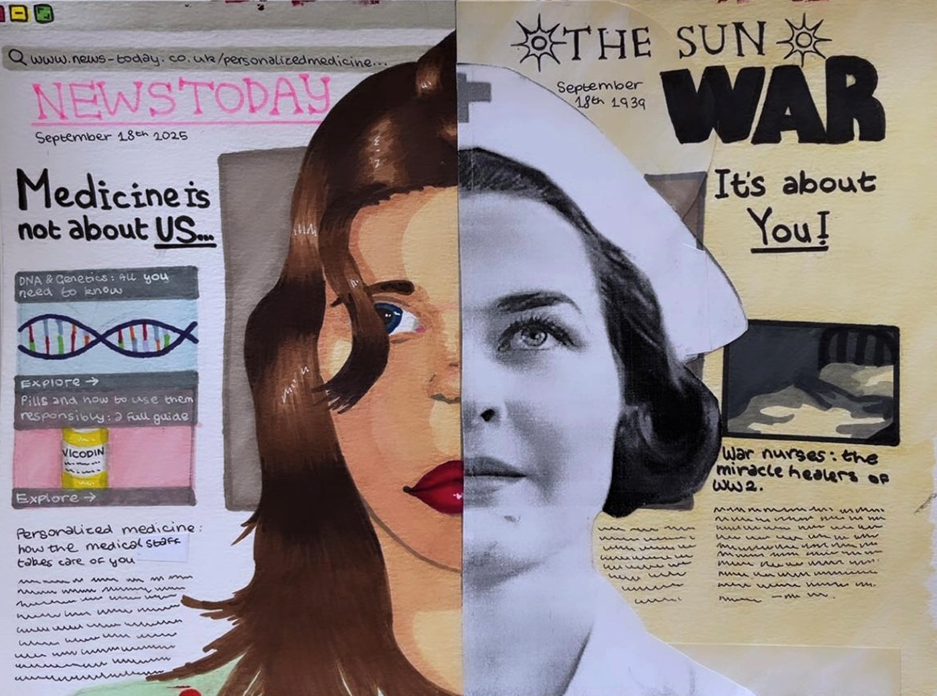
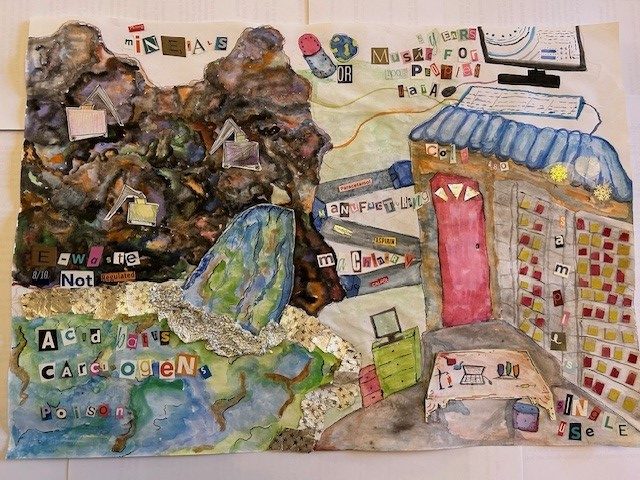
By Ace, age 13, Holland Park School, London
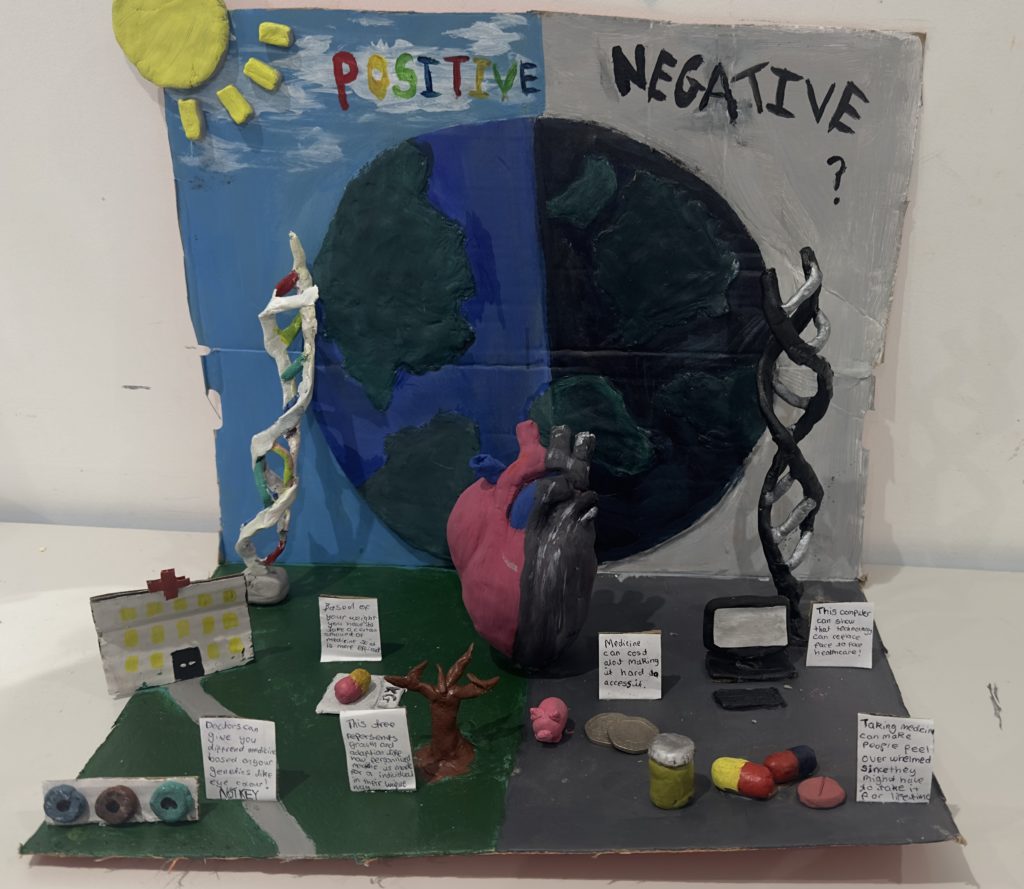
Ace explained ‘I drew this to show the difference between medicine in the past and now. During the war, nurses treated everyone the same, but today medicine is moving towards treatments based on each person’s own DNA and conditions. The idea is to show how healthcare is changing from one-size-fits-all to something more personal.’
The judges thought that this was a visually compelling and original piece, which cleverly brought in historical contexts around medicine and situated personalised medicine within a changing world.
Highly commended:
By Ahsaan, age 12, Magdalen College School, Oxford
Ahsaan explained that his artwork is ‘based on the Vitruvian man by Leonardo Da Vinci that signifies the ‘ideal proportions’ of the human form. I have characterised the Vitruvian man in my artwork, that shows the ideal proportions of personalised medicine specific to our needs and requirements. Depicted around the illustrated figure are the three values that I think make up personalised medicine for me. Predictive, Preventive and a Personalised Treatment. These values all combine and help create a personalised medicine for our individual health which is also what my version of the Vitruvian man is.’
The judges thought this was a fantastic reinvention of the Vitruvian man. We really enjoyed how it drew a strong parallel between Da Vinci’s notion of ideal human proportions and medicine tailored to the individual.
Highly commended:

By Umara, age 14, Guildford High School, Surrey
Umara’s artwork is entitled One Body, One Story. Umara wrote ‘my artwork shows the human body as a jigsaw puzzle, where every person appears whole, but in reality everyone is missing a different piece. The missing piece, (the heart) represents the personal story inside us like our genetics, experiences, emotions and health. Personalised medicine exists to find that missing piece so treatment fits the person, not just the illness. No two bodies are the same, and no two stories are the same.’
The judges thought the use of puzzle pieces was a great concept and very relevant, especially the idea that personalised medicine involves finding ‘missing pieces’.
Winner: group category

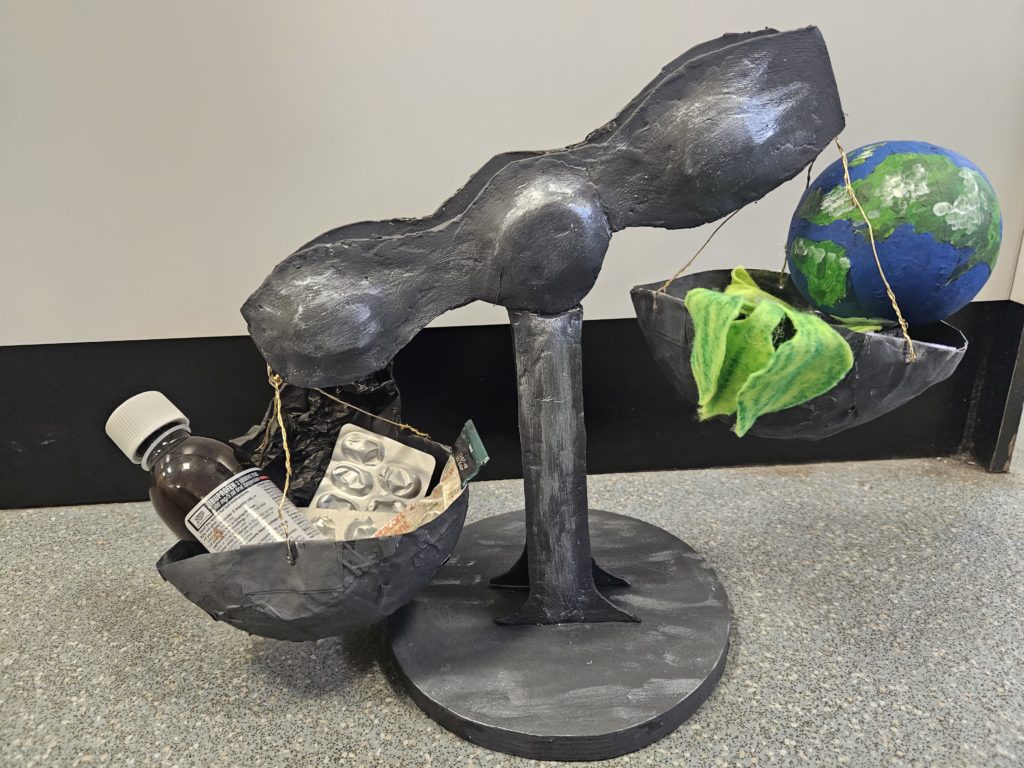
By Cleo & Sadie, age 12, Channing Senior School, London
Cleo and Sadie explained ‘our artwork shows how personalised medicine can affect people’s lives, but not just the lifespan, we tried to capture how medicine can affect your social life, how it can really interfere with your friends, family and education.’
The judges enjoyed how the hourglass brought in the idea of personalised medicine being delivered and experienced over time. The included pictures were very thought-provoking, bringing in a mixture of conventional medical symbols (stethoscope, medication, pills) together with pictures which alluded to the wider contexts of a person’s life. We thought it was a great concept illustrating how personalised medicine might bring both these aspects together across a person’s lifecourse.
Many congratulations to our brilliant winners and finalists, and thank you to everyone who entered or supported the Centre for Personalised Medicine 2025-26 Art Competition. As always it’s been a delight to see the incredible talent and effort that young people have put into these powerful pieces.
We hope to run the competition again next year, so please keep an eye on our website for the details!