Centre for Personalised Medicine Art Competition 2024-25
Earlier this year, the CPM ran an art competition asking UK students in Years 7 to 9 (approx. 11 to 14 years old) to send in art on a theme of ‘how personalised medicine affects our planet’ (click here to see a video introducing the competition).
We were delighted to receive a whole variety of amazing entries. The entries were judged by Dr Rachel Horton (CPM Junior Research Fellow), Dr Ali Kay (CPM Junior Research Fellow), Dr Gabrielle Samuel (Department of Global Health & Social Medicine, King’s College, London), Dr Kate Keohane (St Anne’s College/Ruskin School of Art), Dr Delia O’Rourke (Centre for Human Genetics), Geetika Kumar (Oxford University Personalised Medicine Society), and Raquel Parra (Paintings in Hospitals).
This blog post showcases our winners and finalists, we hope you enjoy these exceptional artworks as much as we did.
Winner: group category
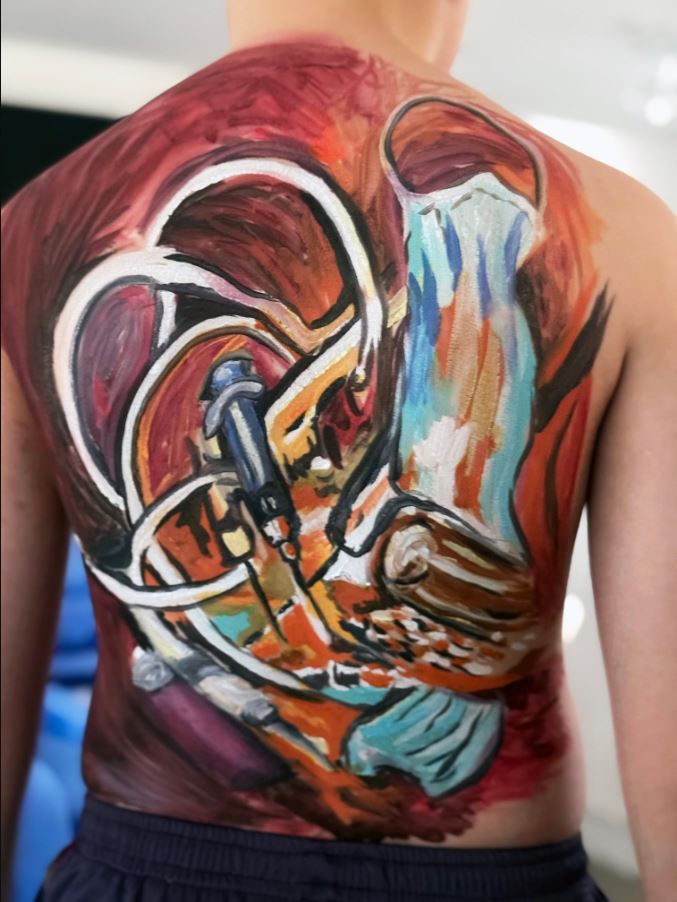
By Charlotte, 12, and Tommy, 11, Mountbatten School, Hampshire
Charlotte and Tommy’s artwork, entitled ‘What we carry’ explores how personalised medicine impacts the environment by showing medical waste painted on a human body. It highlights the amount of single-use plastics, chemicals, and packaging that one person might create through personalised healthcare. By combining the human form with hand-drawn waste, the piece raises important questions about how we can enjoy the benefits of personalised medicine while reducing harm to the planet.
The judges thought that this was extremely original, striking and imaginative – it really brought home the environmental impact of our personal healthcare.
Winner: individual category
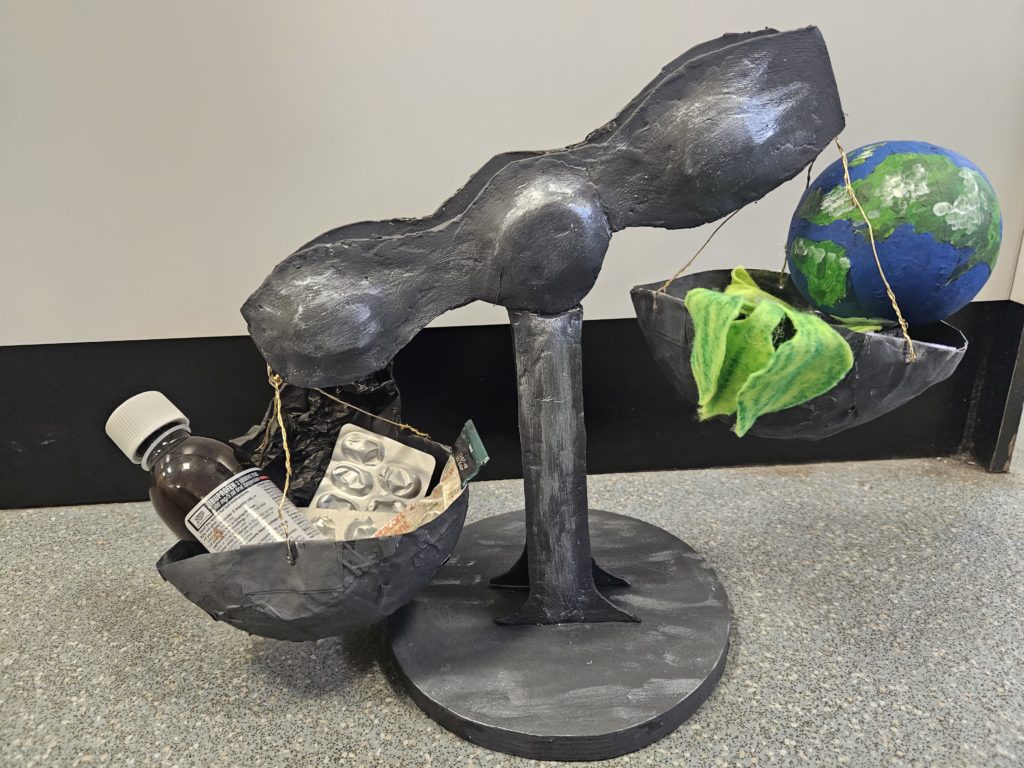
By Owen, 12, Heckmondwike Grammar School, West Yorkshire
Owen’s sculpture shows scales with a medicine bottle, tablets and ointment in one bowl being weighed against our planet and plants in the other bowl, inventively demonstrating tensions between producing medication with the aim of improving human health, and environmental sustainability considerations.
This ambitious and imaginative piece powerfully communicates that there is a balance to be struck between human medicine and the health of the planet. The judges felt that the entry was very creative and a thoughtful exploration of the topic.
Runner up
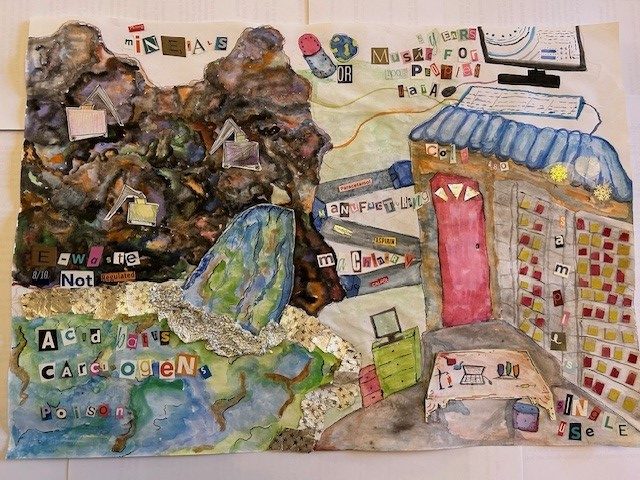
By Hannah, 13, St Helen and St Katherine, Abingdon
Hannah’s artwork ‘Harmful healthcare’ explores how personalised medicine has major consequences on the environment. Hannah explores six different reasons emissions are created when personalised medicine is used: mineral extraction; acid baths; electronic waste; manufacturing and packaging; data storage online; and sample storage. Each of these has a section in the piece which has a water colour representation of what it looks like when it occurs as well as a few concise words which explain what is happening. Hannah used recycled cereal boxes for the waterfall, diggers and desk. All of the letters come from magazine text and the water’s rocks and splash are made out of tin foil.
The judges thought that this considered environmental impacts very thoroughly and showed great use of recycled materials. It showed a diverse range of ways personalised medicine products and practices impact the planet and we loved the mixed media art style and clear message from the piece.
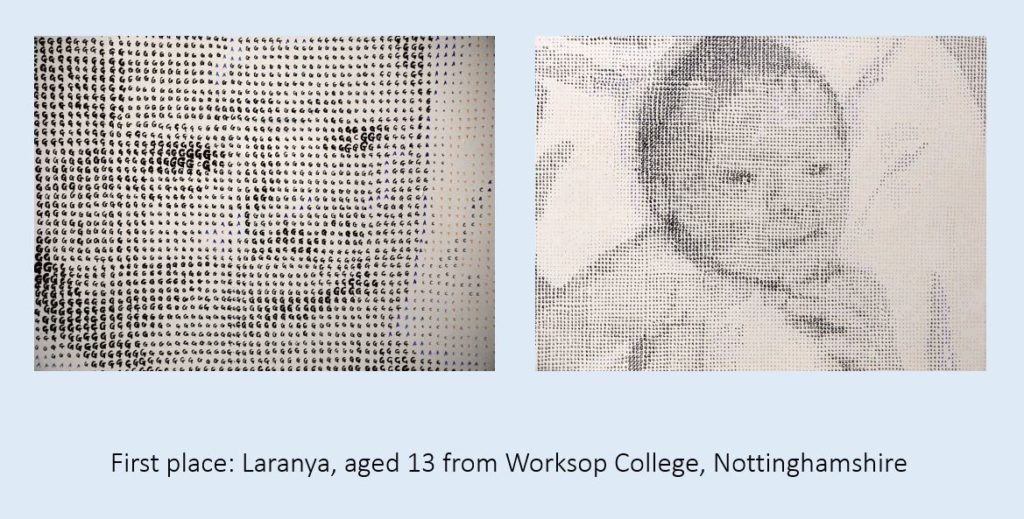
Highly commended

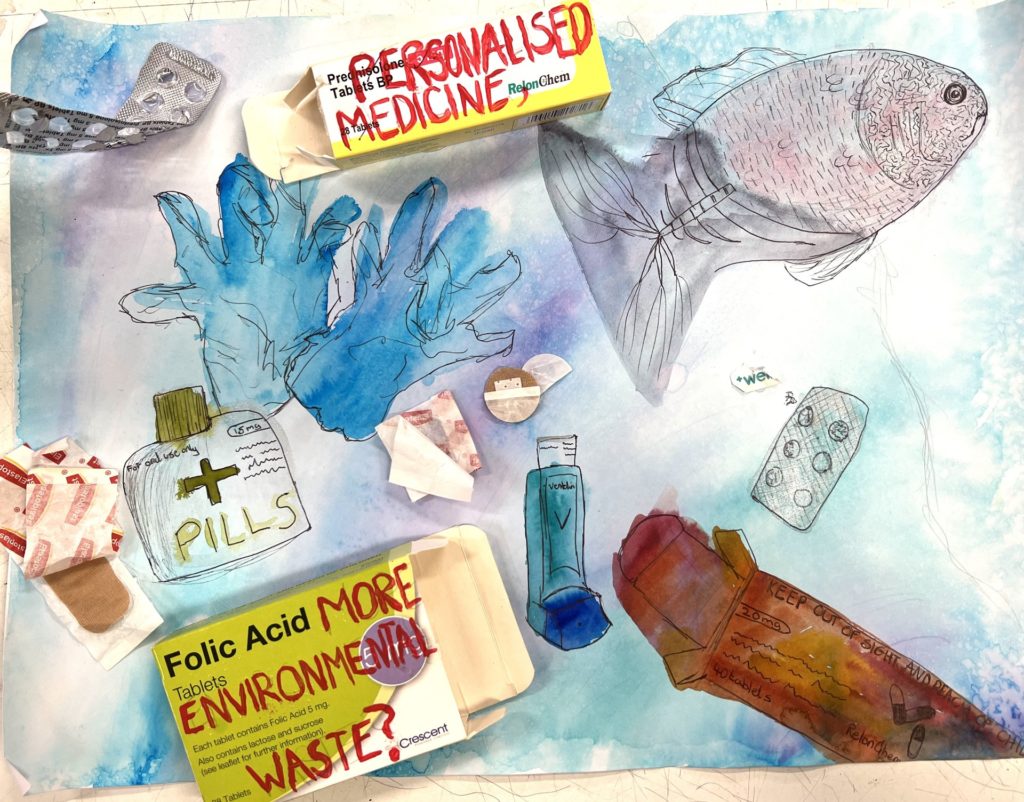
By Laranya, 14, Worksop College, Nottinghamshire
Laranya’s artwork, ‘The Pharmacy Fish’, represents the damage that can take place to our environment for example to our rivers, oceans and wildlife from personalised medicine waste. Laranya layered medicine packets, clinical waste bags, tablets and more in the shape of a fish to express the consequences of the mass production and waste of personalised medicine. She chose specific words such as disposable (encouraging waste), resistant (antibiotic resistance) and others to represent the impact of specific medical activities. The lips are made from disposable thermometers, the lower fins from dental care products. The main fins are from expired Covid tests, syringes and a face mask. The tail and orange parts are from a biohazard bag which is used to collect clinical waste from medical practices.
The judges enjoyed the fantastic use of health-related materials in this collage fish: the colours and textures created are really eye-catching. We thought the entry was extremely thoughtful and relevant regarding the environmental impact of clinical waste.
Highly commended
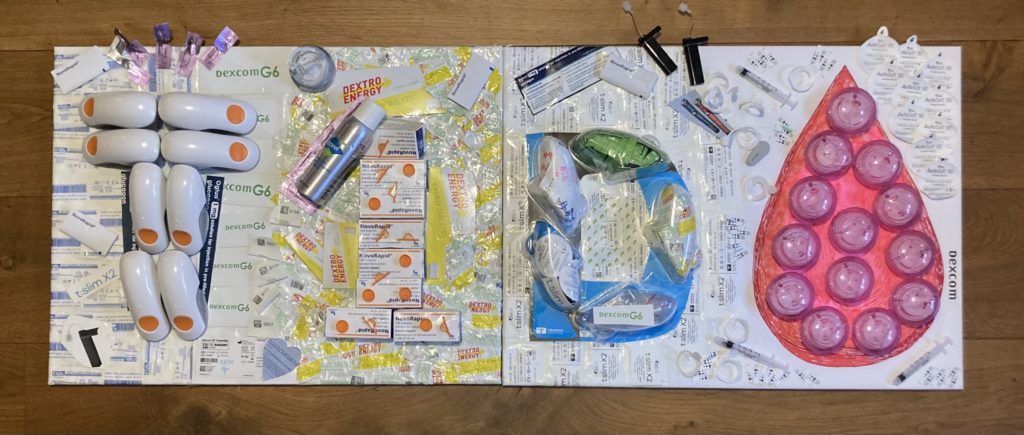
By Matilda, 11, Didcot Girls’ School, Oxfordshire
Matilda’s collage spells out ‘T1D’ – which stands for Type 1 Diabetes – and the drop of blood indicates the number of fingerpricks and injections that people with T1D have to do to keep blood glucose levels in a healthy range. The collage is made from some of the paper and plastic waste materials that are needed to manage health over a three-month period. These materials are the packaging for things like insulin vials, continuous glucose monitor sensors, infusion sets, cannulas and glucose tablets.
The judges thought this was an amazingly creative use of waste material from diabetes care, and a compelling example of how attempts to make medicine more sustainable are clearly really important but must not come at the expense of people’s health. We thought this was a very clever and original artwork.
Highly commended

By Giselle, 13, Harris Girls’ Academy, Bromley
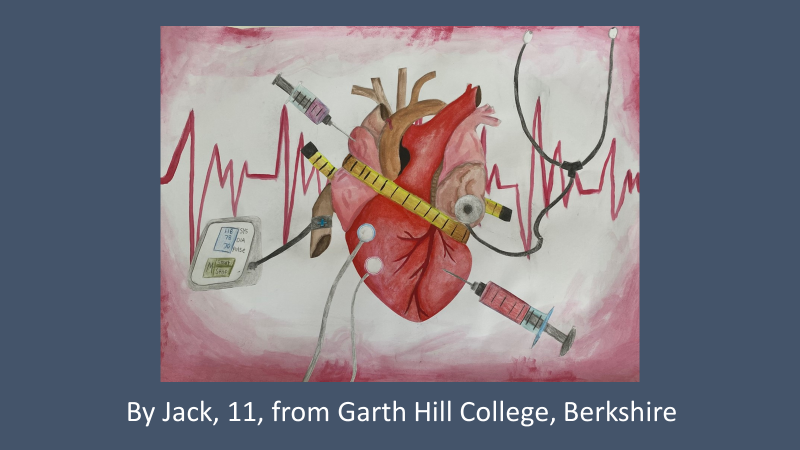
Giselle wrote ‘The shattered pills, tubes and packaging represent pharmaceutical waste. When medicines are disposed of improperly, they enter the environment, contaminating soil and water systems, affecting wildlife and ecosystems. The silhouette of the human figure, combined with the heart and vibrant flower, symbolizes the personal and emotional toll of medicine on the individual. Personalised medicine focuses on tailoring treatments to specific people, but it can also have profound psychological and physical effects, as represented by the heart wound. In summary, my piece emphasises the duality of personalised medicine – its ability to help individuals heal, but also its unintended negative impact on the environment’.
The judges loved how this insightful entry portrayed how personalised medicine might have costs in some areas and benefits in others.
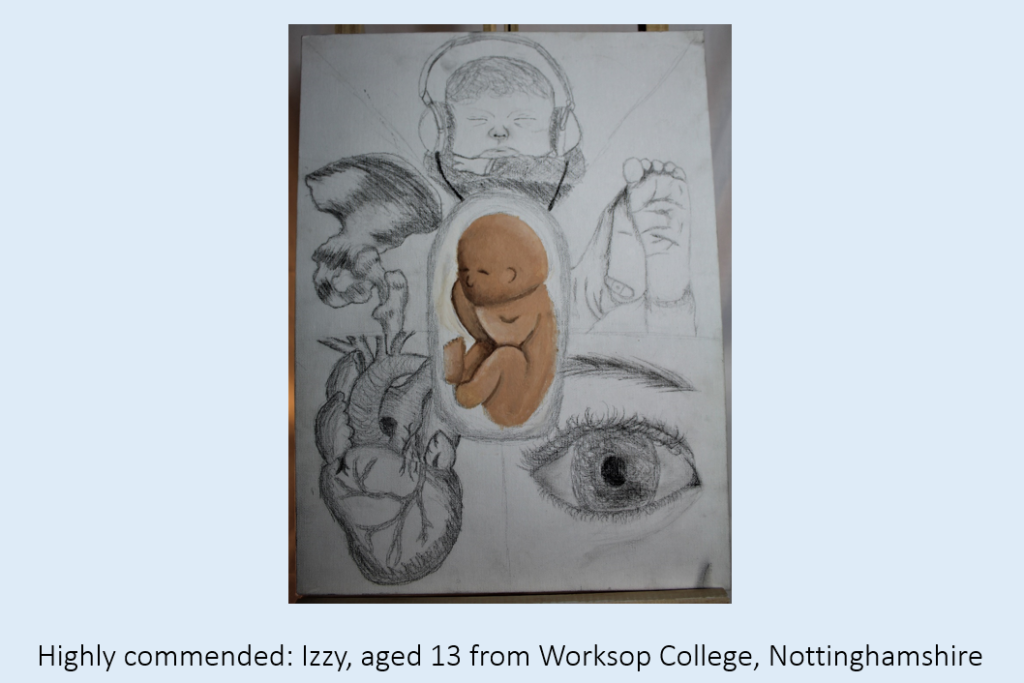
Highly commended
By Evangeline, 13, Worksop College, Nottinghamshire
Evangeline’s art focuses on the impact of personalised medicine waste on aquatic life. The judges enjoyed her skillful drawing and use of collage, and felt this entry was very relevant, direct and original.
Highly commended
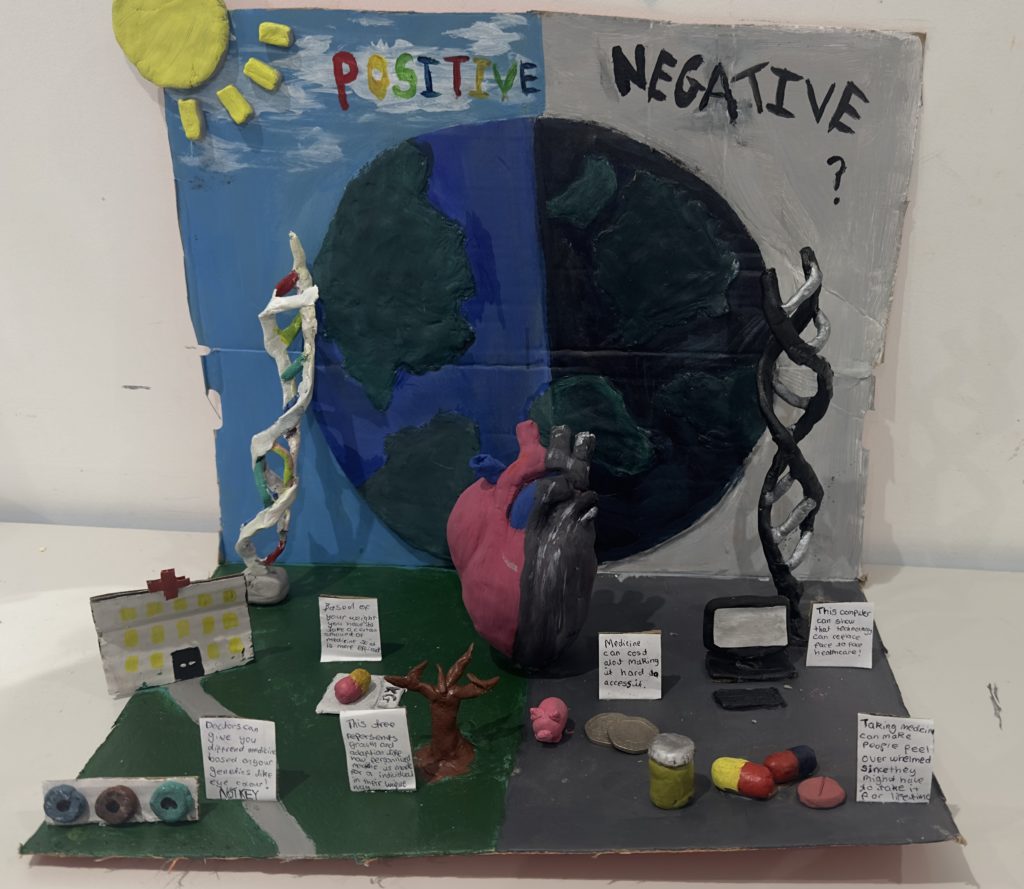
By Kirat, 13, Guru Nanak Sikh Academy, London
Kirat’s engaging sculpture showcases positive and negative impacts of personalised medicine on our planet. The judges enjoyed the 3D model and how it portrayed both opportunities and challenges.
Highly commended
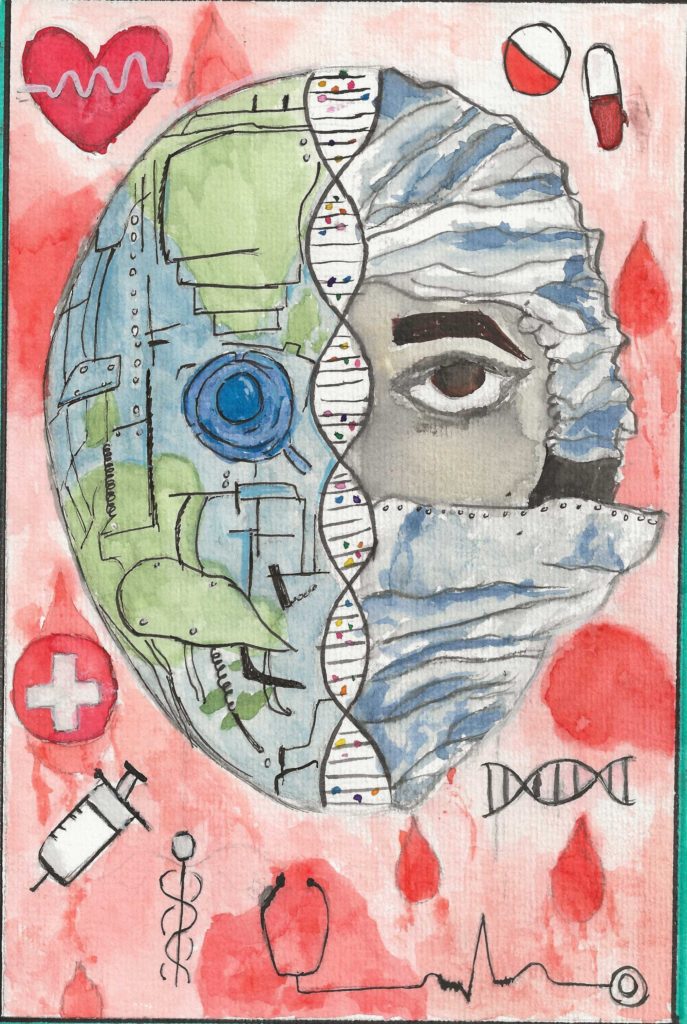
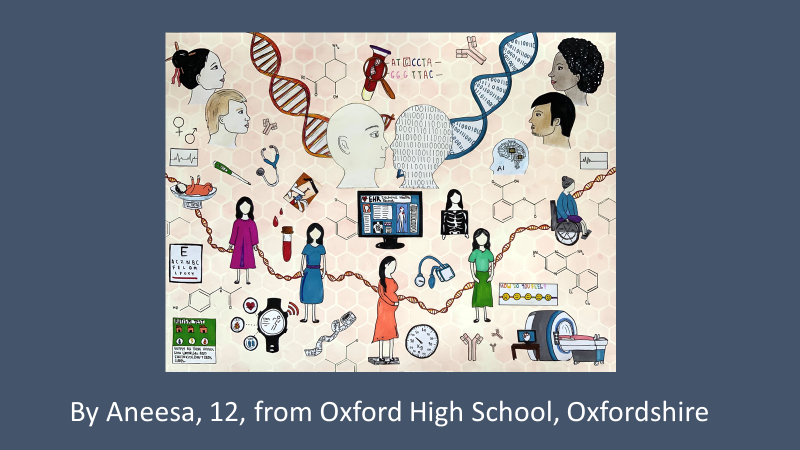
By Saanvi, 12, Wallington High School for Girls, Surrey
Saanvi explained ‘I created a painting on how personalised medicine on the planet is affected by the use of AI. In the middle of my artwork, I depicted a face, split in half, one side a robot, the other a doctor. This represents the state of the world right now as artificial intelligence has begun to take over the research in this field. Research to develop personalised medicine often involves lots of data and working with data uses computers which affects the carbon footprint of the planet. Surrounding the face are detailed DNA double helix structures which resembles the complexity and depth of AI influence in personalised medicine across the planet.’
The judges were struck by Saanvi’s focus on AI and data, and impressed by the level of artistry shown in this entry, which depicts the important connection between the data powering advances in personalised medicine and its impact on the planet.
Many congratulations to our winners and finalists, and thank you to everyone to entered or supported the Centre for Personalised Medicine 2024-25 Art Competition. As always it’s been wonderful to see the incredible talent and effort that young people have put into these thought-provoking pieces.
We’re planning to display these entries at an upcoming ‘Net Zero’ CPM event, and a selection of winning entries from this year, as well as 2022-23, and 2023-24 at the Churchill Hospital in Oxford this Spring. We hope to run the competition again next year, so please keep an eye on our website for the details!